Responses to caries confined to primary dentin
Inflammatory changes of tissues, and also the repair of the phenomenon can be seen in the flesh at all stages of active carious lesions. In fact, tissue responses were seen even at very early stages, before any surface collapse, when caries, is reduced to the enamel only (10, 11, 13).
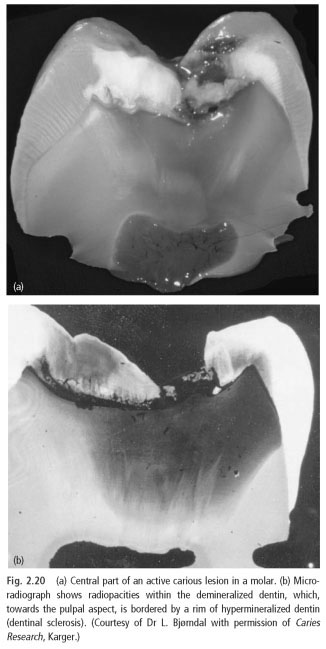
The degree of reaction depends on the number of bacteria stimuli that reach cellulose at a given point. He also is a function of distance. Therefore, while in the periphery, the bacteria release of substances that need to go much further than the defeat near from the pulp. However, the distance factor, as a rule, is of less value when the response processes from the point of view inside the tubular mineralization (dentinal sclerosis) appeared. Dentinal sclerosis makes involved dentinal tubules more or less impenetrable. This is due to the increased secretion of peritubular dentin, which is becoming highly mineralized and reprecipitation mineral crystals, which were dissolved by acids in the carious lesions (11).
These sediments will occur within a limited territory pulpally promotion of demineralizing front (Fig. 2.20). Sclerotic dentin and transparent glass-like appearance. The development of caries process minerals are dissolved and new rainfall can occur in the bone closer to pulp. Therefore, carious lesions in dentin is a dynamic process, which includes the event of a breakdown and remineralization in different parts of the dentin of the body where cavities develops (Fig. 2.20).
It is important to understand that even in its initial exposure dentin caries causes inflammatory reactions in the flesh, i.e. long before the bacteria in the process reached the pulp tissue itself. Support for this view is obtained from experimental studies in humans and animals, where well-known components bacteria in plaque were applied freshly prepared dentin caries (3, 5). Within a few hours, and in Association with the tooth pulp ends exposed dentin, acute inflammatory response developed in the flesh. In these experiments shows that the dentinal tubules really impervious to the elements of bacterial and supports the view that even a small initial carious lesions can lead to inflammatory lesions of the tooth pulp (13).
In the process of growth and cell death of microorganisms in the decaying process, the elements are released, which can trigger a tooth pulp answers, with different mechanisms. They include:
- The penetration of bacteria components which act as antigens and initiators of immune response.
- The release of mediators of inflammation of the cells of the pulp of the tooth, including the odontoblasts (see above).
In located on the periphery of vision odontoblasts and dendritic cells are capable of activating various effector mechanisms of innate and adapative immunity. Highly mobile dendritic cells, after obtaining the protein fragments will move in the regional lymph nodes, and start the primary immune response, which antigen-specific T-lymphocytes are recruited (see Fig. 2.14). On the basis of the carrying Toll-receptors, the pulp of a tooth nerves are also triggered bacterial cell wall elements, such as LPS and teichoic acid (74).
Neutrophils, as a rule, do not get into the pulp at the beginning of dentinal caries. Instead of inflammatory infiltration, most frequently among the macrophages, T-cells and plasma cells. These mononuclear cell infiltrates can be seen or in clusters or scattered in the pulp and paper tissue proper under the carious lesions.
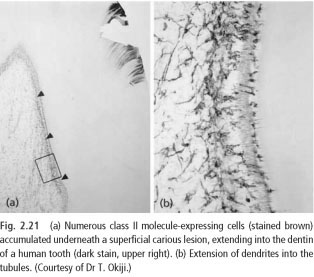
The number of APCS also increases (35), represented by the accumulation of dendritic cells and class II molecules-expressing macrophages (Fig. 2.21). These cells are involved in the secondary immune response, occurring in the pulp and probably in order to strengthen defense and repair of tissues.
Although inflammatory reaction can be expressed in a rapidly progressing caries in young tooth, where the distance cellulose short apparent in adulthood caries, where is progressing slowly. In fact, in the latter case, the activity of inflammatory process is limited and sometimes the only sign of bacterial irritation is the appearance of small rim of reparative dentin (9). The number of the class II molecules of cells expressing also decreased, suggesting that the inflow of bacterial substances in these lesions are reduced or suspended (35). The fact that the fabric change becomes so limited on slowly moved caries is likely to be explained by the previously described reactive processes occurring in the dentin. Thus, it is not excluded, that change of the factors that explain the differences in the tooth pulp responses between fast-and slow-progressing destruction, how intratubular mineralization were deposited to block or reduce the permeability of the affected dentin (11). Formation of reparative dentin and contributes to the reduction of dentin permeability. However, in the periphery of carious lesions of the new dentinal tubules participate and, associated with this, inflammatory/immune reactions and subsequent repair phenomena continue to appear in the flesh.
In the teeth, dental caries, where has progressed over long periods of time, slurries can display intrapulpal and high salinity fibrosis by the neurovascular power. Fabric these changes have less pulp tissue cellular communication and, therefore, less likely to resist the repeated injury.
 ..
..