Activators
The simple inclined plane as a fixed appliance or in conjunction with a removable mandibular plate is rarely used. However, all rigid functional orthodontic appliances operate on the principle of the inclined plane. The activator is the classic functional orthodontic appliance.This is a passive treatment appliance developed by V. Andresen and K. Haupl in the form of a double-plate that is used simultaneously for both jaws.
The regulating effect happens in all three planes of space: Dental arch expansion and narrowing, correction of misaligned individual teeth, and, most importantly, occlusal corrections can be successfully carried out. The appliance fits loosely in the mouth, is not fixed to the teeth, and only works when the teeth are brought together. The appliance impacts the teeth intermittently, and physiologic remodeling stimuli are supplied to the tissues.
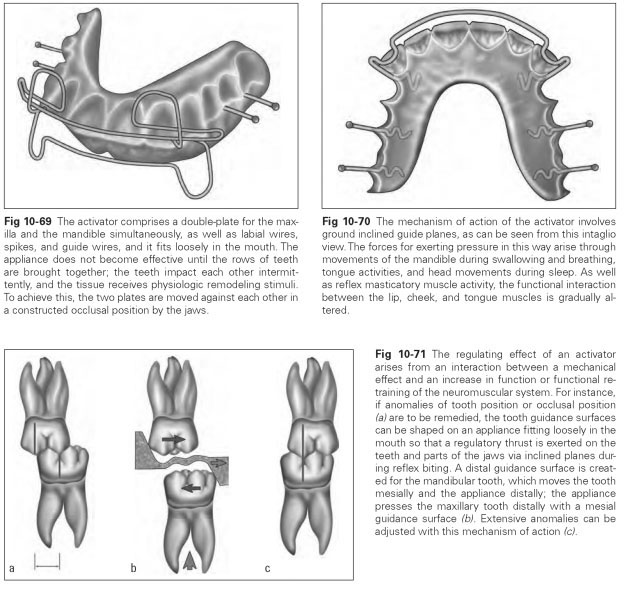
The effect of an activator involves increasing the activity of muscles whose forces are suitable for remedying the malposition of teeth and occlusal anomalies. It works passively by the transfer of muscle stimuli from the masticatory, lingual, lip, and cheek musculature to the periodontal tissue, where it can trigger tissue remodeling. So that the appliance can bring the teeth together intermittently when the patient bites down, the two plates of the maxilla and the mandible have to be moved against each other. The jaws are no longer able to slide into a habitual terminal occlusion but are forced into a different, constructed position. For this purpose, the contact surfaces of the plates with the teeth can be milled out like inclined planes. The activator is first fitted with only a labial bow for the maxillary anterior teeth; spikes and guide wires can also be attached for transverse tooth movement (Figs 10-69 and 10-70).
The passive appliance comprises a reduced palatal plate. This merges into the mandibular plate, which in turn ends just before the floor of the mouth.The two plates are moved against each other in such a way that the lingual impression surfaces of the teeth lie in the proper position in relation to each other. A groove is created for the m andi bul ar anteri or teeth to bi te i nto; th e m axillary incisors do not contact the plate. A labial bow is provided for them. When the patient bites down, the mandible is pulled forward, the posterior teeth are blocked, and the maxillary anterior teeth contact the labial bow. Each individual tooth is now touched by the appliance in such a way that it tips in the desired direction. The maxillary and mandibular posterior teeth have plate contact only at the lingual surfaces, with the activator surfaces being inclined like an inclined plane to enforce tooth movement in the vestibular direction. The activator may additionally be shaped so that the inclined surfaces contact the maxillary posterior teeth not throughout the entire lingual surface but only in the mesiolingual segment, the intention being to stimulate distal movement of the posterior teeth.
The occlusal surfaces of the posterior teeth are avoided so that vertical tooth movement is forced toward the occlusal plane.The mandibular anterior teeth are combined in a block by the in-terocclusal splint and thus held in their position. The maxillary incisors are retruded by the labial bow when the activator is palatally reduced. Biting together also pushes the labial bow against the maxillary anterior teeth and produces the impulse-type forces to stimulate reshaping of tissues.
The following regulating thrusts occur (Fig 10-71):
- Posterior dental arches are expanded.
- Maxillary posterior teeth move distally.
- Posterior alveolar processes are lengthened.
- Maxillary anterior teeth are retruded.
- The mandible is pulled forward.
- Joint changes and alveolar tissue changes are stimulated.
In this process, the remodeling stimuli arise not through continuous pressure but through the appliance being moved during muscle activity. The displacement of the mandible compared with the habitual resting position as a result of activator plates moved against each other is crucial because a regulating thrust occurs with every reflex movement of the mandible. Adjustment efforts can often be undertaken more quickly and more precisely with other orthodontic appliances but not as gently as with an activator. Sagittal occlusal correction is not accomplished as reliably with any other appliance or with such absolute simplicity as with this functional appliance.