Gothic Arch Tracing
The centric position is established with a Gothic arch tracing (intraoral interocclusal record registration) by a method developed by Gysi, Mc-Grane, and Gerber. This arch is formed when the horizontal border movements of the mandible are traced. A tracing stylus is attached to a baseplate and inscribes the horizontal mandibular movements on the tracing plate of the other baseplate. The advantage of this method is that it cancels out all uncontrollable occlusal contacts and reduces them to a central point. At the same time, a relaxed neuromuscular resting position can be adopted in which the joints are relieved of any loading.
For practical purposes, well-adhering baseplates are prepared (for edentulous jaws, on functional models). After a preliminary interocclusal record registration, to establish the correct occlusal height, the maxillary occlusion rim is shortened by about 5 mm, and the maxillary tracing plate is waxed on. The lower stylus holder is placed on the mandibular occlusion rim so that the stylus is exactly in the midpoint of the baseplate. The registration kit should be attached exactly centrally over the jaws so that tilting of the mandible is ruled out and the TMJs are able to balance each other (Figs 8-32 and 8-33). Both plates, the maxillary as well as the mandibular, have side grooves that must be extended in the occlusion rims. This provides retention for the subsequent encoding.
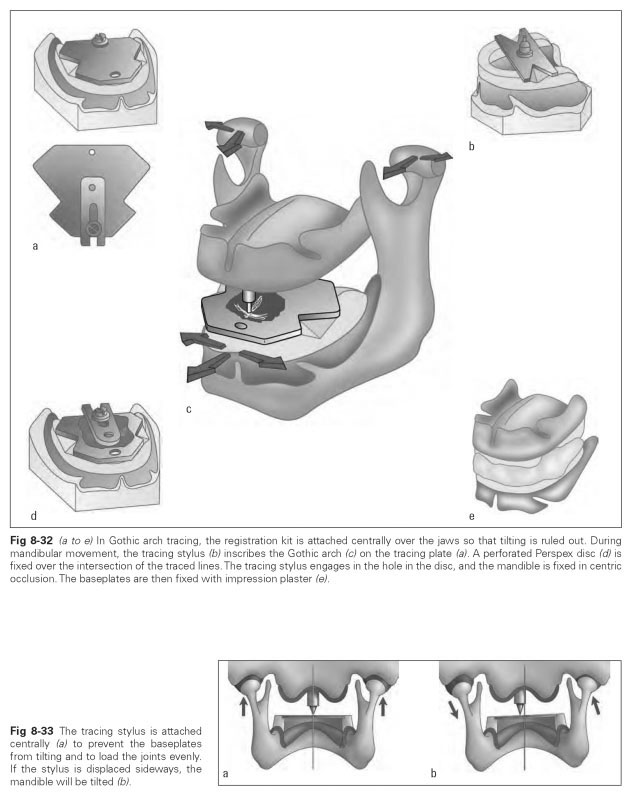
The baseplates are inserted into the mouth to check whether the stylus has the correct occlusal height setting. It can be reset, if necessary. On the tracing plate, a thin layer of wax (or color layer) can be applied in the contact area of the stylus, into which the stylus traces the mandibular movements. The patient makes protrusive, retrusive, and lateral movements several times, whereby the protrusive excursions create sagittal lines and the lateral movements create arcuate, transverse lines that produce the Gothic arch.
The apex of the Gothic arch indicates the most retruded contact position. In healthy TMJ conditions, the centric occlusion position lies about 1 to 2 mm behind the apex of the Gothic arch. Once protrusive and lateral movements have been performed several times, a perforated Perspex disc is screwed onto the tracing plate over the resulting Gothic arch, with the drill hole over the apex of the Gothic arch.The mandible is now directed until the stylus engages in the drill hole. This means the centric occlusion position has been found, and the baseplates are "encoded" (with impression plaster).
The centric occlusion is found, and the degree of possible backward movement during lateral excursions is determined. The condyles rest in the "zenith" of the mandibular fossae without pressure or tension, if the mandible is not tilted dorsally or laterally. The different shapes of the Gothic arch provide information about pathologic forms of movement, joint damage, or muscle spasms but are not diagnostically conclusive. Only the centric occlusion can clearly be established.
Electronic pantography denotes a computer-assisted registration method for the habitual intercuspation position and all mandibular movements in the patient. With a special registration kit (pantograph), the movement of the mandibular incisal point relative to the movement pattern of the condyles of both TMJs is plotted by the computer. The technical procedure involves fixing the registration kit to the patient's maxillary and mandibular teeth so that the relative movement of the mandible is plotted. At the same time, the exact position of the mandibular incisal point relative to the rotation center on the condyles is measured with a facebow and stored on the computer. To transfer the values to the articulator, the models of the occlusal situation are mounted in the articulator with a facebow. The registration kit is fixed on the models as previously in the patient, and the position of the mandibular incisal point relative to the rotation center of the articulator is measured. The computer plots the difference in the values on the patient and on the articulator; transfer and measuring errors are registered by the computer and compensated for mathematically.
Based on the situation of the models in the articulator, the computer calculates the shape of the condylar paths (with the condylar path inclination and Bennett angle) and the anterior guidance path and has these movement paths milled into acrylic blocks in the milling machine. These blocks are then clamped into the articulator.