Advantages of fixed appliances
- Can be used universally.
- Almost any correction aimed at an ideal arch form can be performed.
- Treatment period is relatively short (even in severe cases) and clear and manageable for the patient.
- All the auxiliaries are prefabricated and can be placed directly in the patient by the dentist.
- Corrections can be made immediately and directly in follow-up appointments.
- Patient cooperation is not required to ensure compliance.
- No damage to the appliance due to improper handling by patients.
- Treatment program is direct with straightforward planning.
Disadvantages of fixed appliances
- The amount of force cannot be objectively monitored.
- The appliance acts continuously with no interruption.
- Tissue damage, such as root resorption and shortening of the alveolar ridges, is possible.
- Limited cleaning ability with an increased risk of caries.
- Frequent radiographic checks are necessary.
- Multiband appliances or bonded brackets have an adverse impact in the social context.
Multiband technique
The mechanism of action of fixed appliances is based on an archwire being fixed in the brackets under tension. When the archwire is relaxed, it pulls the teeth in the direction of relaxation. The arches are made of thin and highly flexible wire that bridges the distances between the individual brackets. If the archwires are too thick, the periodontium might be damaged; if the elasticity of the wire is exceeded, it could be permanently deformed and become ineffective.
The principle of treatment involves controlling the orthodontic movements of the teeth with increasingly strong wires and bringing the teeth into the desired ideal position. The intraoral archwire is activated or the next-stronger archwire is inserted.
Activation is achieved by specific bending of the inserted wire to bring about horizontal changes of position, vertical shifts of position, or rotation movements.
The treatment phases of multiband techniques relate to the changes of tooth position:
- Leveling phase involves eliminating vertical and horizontal positional anomalies.
- Guidance and contraction phase involves movements along the arch for space closure.
- Idealization phase means aligning all the teeth in the ideal position.
- Retention phase takes place over a prolonged period after the active treatment is completed.
The direction of pull and hence the direction of movement of the teeth is always toward an ideal dental arch because, when the archwire is relaxed after the treatment, it resumes the ideal form it had before being put under tension.
The brackets are the precisely fitting guide splints for the wires, similar to the components in slide attachments but with wider-fitting tolerances. These guide splints are formed as half-tubes for the round wires or as square slots for square wire (Figs 10-83 and 10-84).
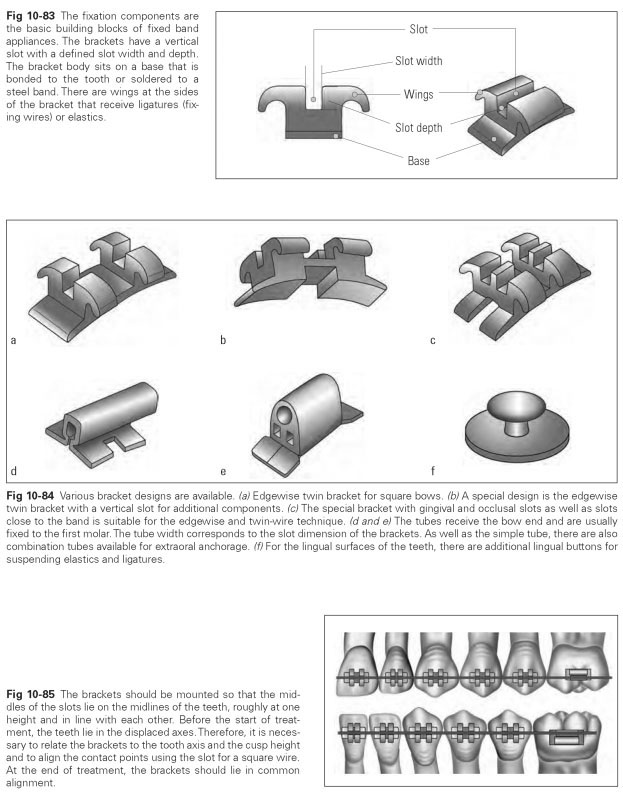
The positioning of brackets on the vestibular surfaces of the teeth is done so that the guide splints are vertical to the tooth axis and at the height of the contact points. The brackets are attached so that they lie at the midlines of the teeth, almost at a single height and in line (Fig 10-85). Before the start of treatment, the teeth are in their shifted axes. Therefore, the brackets need to be related to the tooth axis, and the guide slot for the square archwire needs to be aligned with the contact points. At the completion of treatment, the brackets should lie in common alignment. Attaching the brackets is the most important aspect of using fixed orthodontic appliances because this determines the eventual tooth position. Singletooth movements along the archwire or tipping parallel to it can also be carried out. If a space needs to be closed, the teeth to be corrected can be moved by elastics because the brackets are not only joined to the archwire but also linked to each other with elastics. The brackets and hence the teeth are pulled along the archwire.
Selective movement is possible when several anchor teeth are firmly fixed to the wire and the tooth being moved is flexibly connected to the wire. If a tipped tooth is to be aligned, a spring can be incorporated into the bracket and hooked onto the archwire under tension. Then the tooth being aligned is not connected directly to the archwire but indirectly via the spring.
Discrepancies of occlusal position can be remedied by elastics under maxillomandibular tension. If the elastics are stretched between individual antagonists, an open bite can also be corrected. A tooth twisted in the dentition can be pulled into the normal position with elastics that are attached lingually to the tooth (via lingual cleats) then guided to the archwire.
The palatal (or maxillary) expansion appliance is a fixed active appliance comprising four orthodontic bands and an expansion screw that is cemented in place in the mouth. It rapidly pushes the halves of the maxilla apart within a few weeks and causes a fracture in the narrower area of the midpalatal suture. The aim is expansion in cases of a severely constricted maxilla with a unilateral or bilateral reverse articulation; at the same time, the nose is widened. In the process, the mucosal coverage of the oral and nasal cavity as well as the periosteal covering remain continuously intact. The fracture gap that is opened and kept open fully heals in about 6 months.
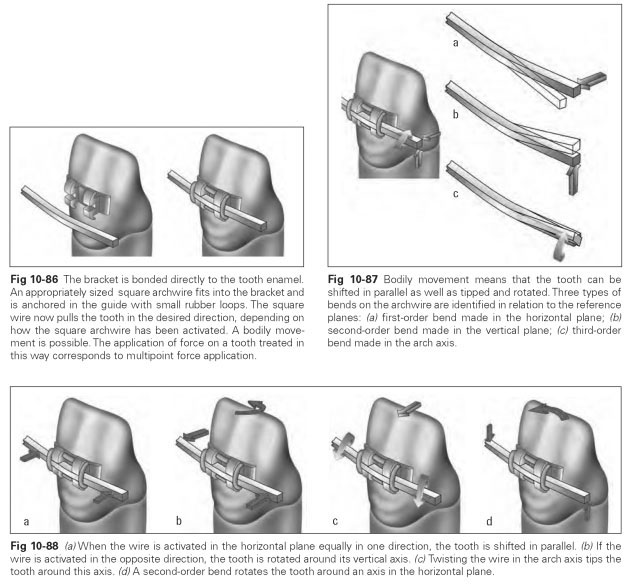
Figures 10-86 to 10-88 illustrate principles of the multiband technique.