Fully Edentulous Maxillary Tissue Integrated Prosthesis Using Porcelain-Fused- To-Metal
The critical factors in the use of porcelain are: meticulous fabrication and laboratory maintenance of a precision framework. It is imperative that correct procedures be followed continuously through to completion of the prosthesis. The design of the substructure should incorporate accurate anatomical dimensions with strong, rigid connectors. In a full-arch framework, a palatal bar is included in an effort to prevent warpage. Thin areas of metal are avoided in all ceramo-metal frames. This minimizes flexure and metal fatigue, both leading to potential porcelain fracture. The Branemark System gold cylinder has a melting temperature of 2350° F, and any metal selected for use must be well below this temperature. The castable components in the Core-Vent and IMZ systems permit the use of base, noble, or high noble alloys.
Ideally, the porcelain veneer should be 2 to 2.5 mm thick in order to insure a high compressive strength. With proper framework design, facilitating optimum porcelain veneer coverage, the restoration has a high degree of rigidity. 2 This allows even distribution of occlusal loading forces to the osseointegrated fixtures.
With the exception of areas of weak trabecular bone,3 there are no significant studies which prove that the lack of shock-absorbing qualities inherent in porcelain should contraindicate its use as a treatment modality. In the event that a porcelain restoration is ultimately required when there is trabecular bone, a period of controlled loading should be prescribed, using an acrylic resin prosthesis.4 Bone remineralization has been observed occurring up to one year after fixture placement in the mandible, and up to 18 months in the maxilla.s Bone remodeling continues for many years. Using an acrylic provisional provides a damping effect which allows additional dense lamellar bone to form. This gives the fixture an increased resistance to overloading, increasing the probability of a successful ceramic bridge.
Minimal resorption of the alveolus in partially edentulous mandibles, and the restrictive space limitations present in the anterior of the maxilla, often requires a ceramo-metal restoration. The use of custom shade matching and oral hygiene maintenance, along with the qualities of resisting staining and occlusal wear, are potential favorable characteristics of a porcelain restoration.
This master impression contains seven impression copings. Before attaching the brass replicas with guide pins, each coping is closely inspected for debris present on the surface.
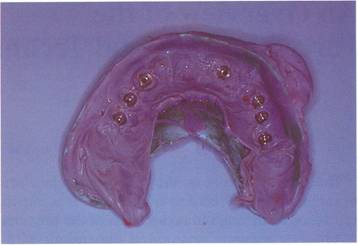
The master cast is poured with improved die stone. A full arch impression should be extended to duplicate good ridge morphology and anatomic landmarks.

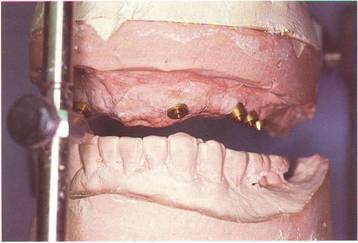
The maxillary and mandibular casts are articulated.
A clear acetate vacuum-formed matrix taken from a model of the patient's temporary restoration is fitted to the articulated upper cast using the palette as a guide.

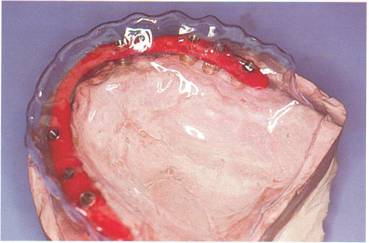
DuraLay resin is used to connect the gold cylinders on the lubricated maxillary cast.
When the acrylic has the desired thickness of 4 mm, the clear matrix is used to establish buccal, labial and lingual borders. Excess acrylic is trimmed until the matrix will seat easily on the model.
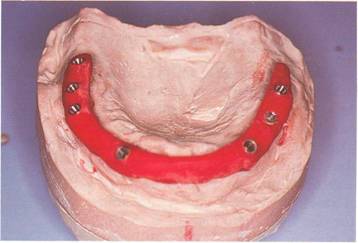
The acrylic is cut into four sections, and each section is waxed to final contour using the clear matrix as an anatomic guide. After all wax has been added, the pieces are joined together with fresh resin and allowed to bench set for one hour. A palatal bar is added with a #8 gauge sprue attaching the distal molars. This bar will help the frame resist distortion from the heat and stress of the porcelain oven.

After careful investing with a high heat investment (Ceramigold, Whip Mix Co.), the ring is allowed to bench set for one hour, it is then placed in a cold burn-out oven and the temperature raised to 5000 F and held for one hour. The oven is reset for 1450° F and again held for one hour. The pattern is cast in a high noble alloy (WY, Williams Co.) and allowed to bench cool. The metal frame is then cleaned and finished. During metal finishing, it is very important that brass replicas or similar components be fastened to the cylinders with guide pins. This preserves the integrity of the cylinders and encourages a fine finish line at the junction of the frame and cylinders. This procedure is repeated for any additional metal work and also for the final polishing of the frame.

At the metal try-in stage, the frame does not fit passively on all fixtures.6 The metal is sectioned through the left central and the palatal bar, both pieces are reseated with gold screws, and a DuraLay index is made for soldering. A solder model with brass replicas is made from the indexed frame. Using the frame as an index, the inaccurate brass replicas are removed from the master cast. New brass replicas are fastened to the frame with guide pins and refitted to the master cast, making sure that no stone is in contact with the brass replicas. The frame is secured with guide pins and stone is poured around the new replicas. This completes the altered cast technique. The case is then removed from the new master cast, invested with high heat solder investment, and soldered (see Chapter 10). The metal is then cleaned, finished, and returned for a second metal try-in.

A lateral view cephalometric radiograph verifies the intimate and passive fit that is required from the frame.

After the frame has been degassed and the custom opaque applications are complete, the gingival and incisal porcelains are built up. Full cervical contour is evident, along with slightly lengthened incisal edges. The porcelain must be contoured and condensed accurately on the first bake. Multiple firings of full arch porcelain prosthesis increase the chance of frame distortion.
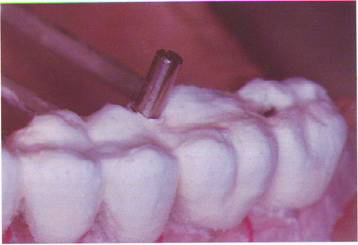
The guide pins used during the porcelain buildups maintain the cleanliness of the screw and cylinder interface. After baking, the ceramic particles are very difficult to remove from the inside portion of the cylinder.
A bisque bake trial is completed, with some adjustments being made to equilibrate the occlusion.
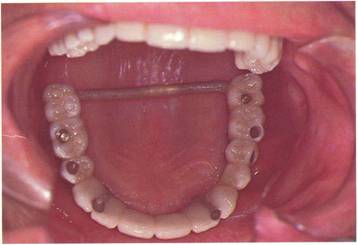
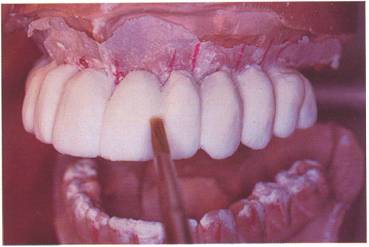
The porcelain is then glazed and the metal is polished. The palatal bar is cut off at this time and the prosthesis is screwed into place, with the access holes temporarily sealed with cotton pellets and cavitt.
Prosthodontic rehabilitation is now complete, with full muscle support evident in the cheek and lip area.
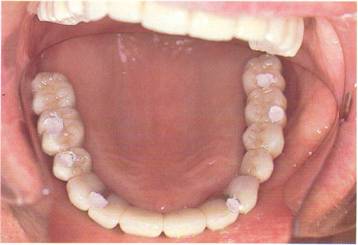
Lip retractors reveal good soft tissue adaptation and all screw access holes cosmetically hidden from view.
