Anatomy of the oral cavity
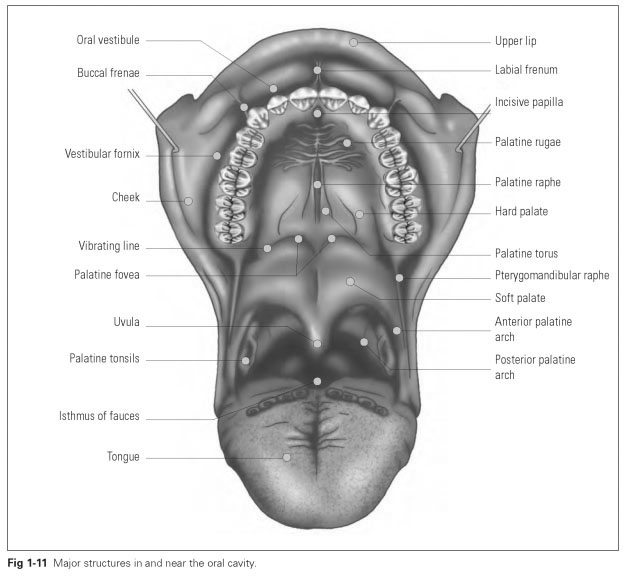
The oral cavity is the space between the orifice of the mouth and the isthmus of the fauces (isthmus faucium; also called the oropharyngeal isthmus) (Fig 1-11). The
alveolar processes, which bear the teeth, divide the oral cavity into the oral vestibule (vestibulum oris) and the oral cavity proper (cavi-tas oris propria), the mucosa of which is covered by stratified squamous epithelium.
The oral cavity proper is formed by the oval space behind the dental arches and is almost fully occupied by the tongue. The palate, which is like a roof, marks the superior boundary of the oral cavity; the other boundaries are the isthmus of the fauces posteriorly and the floor of the mouth below.
The floor of the mouth lies between the parabolic mandibular body and extends as far as the root of the tongue. It is the muscular base of the oral cavity, being formed by some of the suprahyoid muscles of the hyoid bone, mainly by the mylohyoid muscles (musculus mylohyoidea; running from the mandibular body transversely to the midline of the skull), on which the tongue rests. Above and below these muscles are the sublingual and submandibular salivary glands. The boundary of the floor of the mouth is shaped laterally by the mylohyoid line and anteriorly by the movable sublingual area. This limited sublingual space is often referred to as the floor of the mouth. Sublingual and submandibular salivary glands are found in the floor of the mouth.
The palate (palatum) is the roof of the oral cavity. It is divided into the hard palate (palatum durum) and the soft palate (palatum molle), which consists of the movable velum palatinum and ends at the uvula. The hard palate also forms the floor of the nasal cavity and the maxillary antrum.
The bony foundations of the hard palate (palatum osseum) are the incisive bone (os incisivum) anteriorly, the palatine processes of the maxillae (processus palatinus), and the horizontal plates of the palatine bones (lamina horizontalis).The hard palate is covered with mucosa, which is attached to the periosteum by bands of connective tissue. The firm attachment of the mucosa to the underlying bone means that the tissue is not displaced during mastication.
Over the median palatine suture (sutura pa-latina mediana), the mucosa of the hard palate forms a midline elevation, the palatal raphe (raphe palati mediana), which starts behind the incisor teeth at the incisive papilla (papilla incisiva) at its tip and may show a protuberance known as the torus palatinus in the middle of the palate. The incisive papilla lies over the incisive foramen (foramen incisivum) of the bony palate and is protuberant. Below the papilla, blood vessels and nerves emerge from the incisive canal.
In the anterior part of the palate, a few irregular mucosal ridges emanate from the raphe: these are the palatine rugae (plicae palatinae trans-versae). Along with the firmly attached mucosa, they help create friction between the palate and the tongue to help in mastication and speech; the moving bolus of food does not displace the mucous membrane, and the tongue is able to turn food over and let the saliva infiltrate it. The rugae are made up of a network of connective tissue fibers and isolated cartilage cells. An accumulation of tactile nerves is found here. So that food can slide along in the rear part of the hard palate during swallowing, this area contains the palatine mucous glands (glandulae palatinae) and is padded with fatty tissue. These glands become more numerous toward the soft palate.
The vibrating line denotes the transition from the hard palate to the soft palate. It is a line formed into a double arch that runs from one maxillary tuberosity to the other and encloses the posterior nasal spine.To the left and right of this line are the foveae palatinae, which are openings for the palatine glands.The vibrating line can be identified by producing a nose-blowing effect and generally forms the posterior border of a denture. This line is usually etched on the cast to mark the peripheral seal of the denture. Thus, the maxillary denture should end in the area of transition between the hard and soft palates, which results in a peripheral seal and ensures that no air enters between the fitted surface of the denture and the palate; in this way, the denture is kept in place by suction.
The soft palate, continuing from the hard palate, is a mucosal fold filled with muscles and a solid connective tissue framework, the superior surface of which forms the posterior floor of the nose.The highly mobile posterior part of the soft palate is known as the velum palatinum, and it terminates in the midline as the uvula, which is a continuation of the palatal raphe. The sides become the palatine arches or pillars (arcus palatini).
The muscles of the soft palate are the tensor veli palatini, levator veli palatine, musculus uvulae, palatoglossus, and palatopharyngeus. These muscles are able to pull the velum palatinum posteriorly as far as the root of the tongue so that the oral cavity is sealed posteriorly and airtight. With the mouth closed, the mandible can thus be held in its resting position by the pressure of air; normally it is kept in this position by resting muscle tension (tonus). The palatine glands are found on the inferior surface of the soft palate (toward the oral cavity). These are mucous glands, just as in the hard palate area, which enable the food to slip down smoothly when swallowing. The soft palate, with the palatine arches or pillars at the sides and the root of the tongue, forms the isthmus of the fauces. Between the two palatine arches lie the palatine tonsils (tonsillae palatina). When the soft palate is touched, it can trigger a gag reflex.