Malposition of teeth in the sagittal plane
Occlusal anomalies in the sagittal direction can be described as malocclusions according to Angle's classification. Starting with neutro-occlusion (Class I), a distinction is made between unilateral or bilateral disto-occlusion (Class II) and unilateral or bilateral mesio-occlusion (Class III).
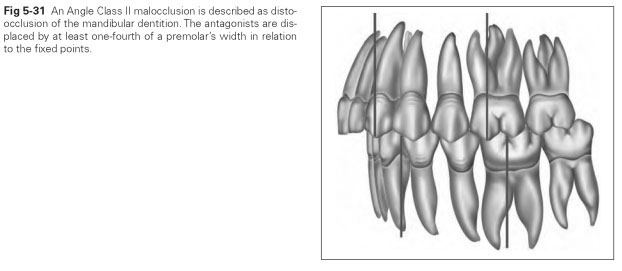
Disto-occlusion or posterior occlusion means retrusion of the mandibular teeth in relation to the fixed points: The maxillary canine and the
maxillary first molar are pushed anteriorly by one-fourth of a premolar's width from the position of neutroocclusion (Fig 5-31). All possible malpositions of individual teeth can be seen here. One noticeable defect of this occlusal displacement is the position of the anterior teeth in relation to each other. This gives two more groups of divergent anterior relationships.
The anterior open bite with protrusion of the maxilla (Angle Class II, division 1) takes the following forms:
- Labial tipping of the maxillary incisors
- Lingual tipping of the mandibular incisors
- Lengthening of the maxillary dental arch (tapered front)
- Shortening of the mandibular dental arch to produce a flattened front
- Sagittal overdevelopment of the maxilla (prognathism)
- Sagittal underdevelopment of the mandible (mi-crognathism)
In combined forms, the vertical overlap of the incisors can be very large so that the lips are not closed when in their relaxed position, and the incisal margins of the maxillary anterior teeth lie in front of the bottom lip. The resultant open-mouth breathing affects the bacterial flora in the oral cavity and increases the susceptibility to caries. If the bottom lip presses behind the maxillary anterior teeth when swallowing to ensure an air-tight seal, the protrusion is increased. This dentition anomaly is usually hereditary and less often due to exogenous factors such as thumb sucking, nasal breathing, or incorrect sleeping position.
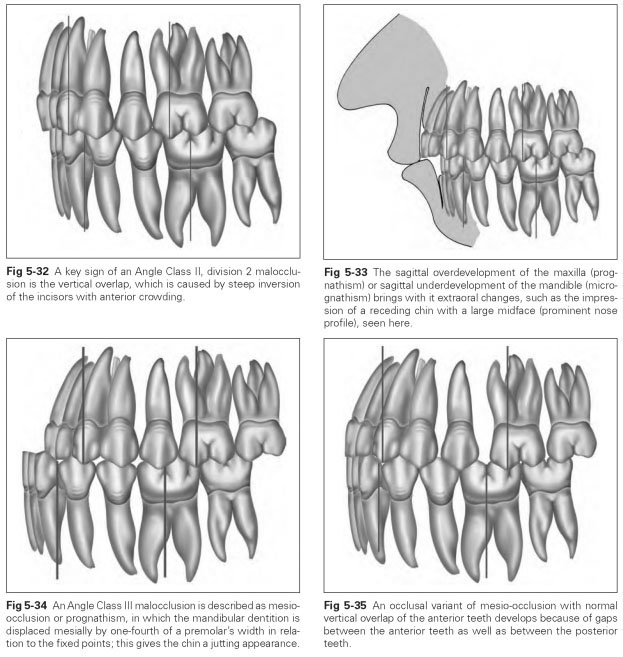
A deep bite or steep bite (Angle Class II, division 2) exists if the maxillary incisors are positioned extremely steeply in the jaw and cover the mandibular anterior teeth to a variable width without sagittal protrusion (Fig 5-32). The more inverted the teeth (tipped inward), the more pronounced is any anterior crowding.The lateral incisors sometimes overlap the central incisors or the canines in a flattened anterior dentition. If the alveolar ridges are lengthened, the maxillary incisors reach the mandibular gingival margin or vestibular fornix. Here both the maxillary and mandibular anterior teeth go beyond the normal occlusal plane. A vertical overlap may also exist in combination with neutro-occlusion. The profile appearance of a vertical overlap is a deepened mentolabial sulcus over a prominent chin and a shortened lower face. It gives the impression of overdevelopment of the midface with a large nose (prominent nose profile) (Fig 5-33). In the case of deep bites, the sideways movement of the mandible under tooth contact is impeded or impossible. The masticatory movements then tend to follow a chopping masticatory pattern. Forward movements lead to excessively wide distances between posterior teeth.
Mesio-occlusion denotes the mesial displacement of the mandibular dentition by at least one-fourth of the premolar's width, in relation to the fixed points (Fig 5-34). The anterior teeth may have a normal vertical overlap, and gaps between the maxillary anterior teeth are common (Fig 5-35); edge-to-edge occlusion, in which the incisal margins of the maxillary and mandibular anterior teeth meet, is possible. If the inclination of the axes of the teeth is correct, this results in protrusion of the mandibular anterior teeth in front of the maxillary teeth. This malposition of the teeth is known as an anterior reverse articulation, reverse vertical overlap, or mandibular protrusion. If brought into the neutro-occlusion position, a mesio-occlusion can have entirely normal intercuspation of the posterior teeth and incisors with a normal vertical overlap.
Prognathism denotes the sagittal protrusion of the mandibular anterior teeth without the presence of mesio-occlusion. The extraoral symptom of prognathism is a pronounced, protruding, prominent chin, hence the alternative name progenia (geneion = chin). Prognathism can take the following forms:
- Tipping of the maxillary anterior teeth in a palatal direction
- Tipping of the mandibular anterior teeth in a labial direction
- Lengthening of the mandibular alveolar arch
- Shortening of the maxillary dental arch to produce a flattened front
- Overdevelopment of the mandible in a sagittal direction
- Underdevelopment of the maxilla (microgna-thism)
The degree of prognathism ranges from an edge-to-edge position of the anterior teeth through to the mandibular anterior teeth completely covering the maxillary anterior teeth, which is always associated with a reverse articulation situation. The rows of teeth can cross at the canines or the lateral incisors. In prognathism, the incisal position cannot be adopted or only with force. Sideways movements are possible without slip interferences, provided a reverse vertical overlap is not present. Prognathism is hereditary and can be accentuated by exogenous factors.