Periodontium
The tooth is anchored in the jawbone by a complicated attachment mechanism. Previously it was assumed that the teeth were fused into the bone of the jaw. More detailed analysis of tissue sections, however, revealed a narrow gap between bone and cementum—the periodontal space—in which the tooth is joined to the jawbone by a fibrous apparatus. In descriptive anatomy, this attachment mechanism is called syndesmosis.
Syndesmosis means band attachment, in which the two bony parts are joined together by ligaments. On closer inspection, some movement of the tooth in its bony anchorage can be detected, so that it could be described as an articulated joint in the sense of a synarthrosis (arthron = joint). Synarthroses denote articulations uniting bones with extremely limited movement (eg, dentoal-veolar articulation).
The periodontium comprises all the tissues that anchor the tooth in the bone; ie, it is tooth-supporting tissue (peri = around, odous = tooth; paradontal = near or close to the tooth). This is a functional unit of various supporting tissues. These tissues are seen as a functional unit firstly because they form a single unit once they have developed. Secondly, they belong together in terms of clinical pathology. Thirdly, they form a compact system for the particular task (function) of anchoring the tooth in the jawbone. The bony parts in which the teeth are invested are functionally oriented tissue structures that mature in line with tooth eruption and later can be completely resorbed after tooth loss.
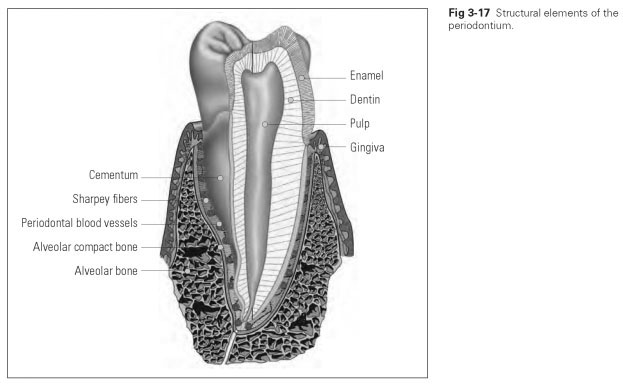
The periodontium includes (Fig 3-17):
- Cementum
- Alveolar bone (os alveolare)
- Periodontal ligament (desmodontium)
The periodontal space is a gap about 0.1 to 0.2 mm wide (when healthy) between the cementum and the
alveolar bone, which is seen as a thin line on radiographs. This is where the
periodontal ligament is located. It is mainly made up of connective tissue fibers that join together to form separate bundles of fibers. These are known as Sharpey fibers. The periodontal ligament also contains blood vessels and nerves.
Sharpey fibers are fused in the cementum and in the alveolar compact bone tissue, the counterpart of the cementum. The bundles of fibers do not run horizontally from the alveolar bone to the tooth but obliquely down to the root, ie, in an apical direction. A few bundles of fibers also run crosswise from the alveolar bone slightly around the tooth to the root and secure the tooth against twisting. During chewing, the tooth cannot be compressed very far into the bone because Sharpey fibers are not elastic.
Masticatory loading presses the tooth into the tooth socket (Fig 3-18). Because Sharpey fibers run apically from the alveolar bone in the direction in which the tooth is being pushed, the fibers are immediately placed under tension. They are not elastic and therefore transfer the tensile stress to their anchorage points in the alveolar bone and cementum. They pull on the hard tissues; ie, the hard tissues are placed under tension during masticatory loading. The ligament apparatus transforms compressive forces into tensile forces.This is an advantage because it is a property of bone tissue to atrophy in response to compressive stress; in response to tensile stress, however, it grows or is strengthened in the direction of pull. The same mechanism applies when the tooth is twisted: the crosswise looped fibers then pull on the hard tissues.
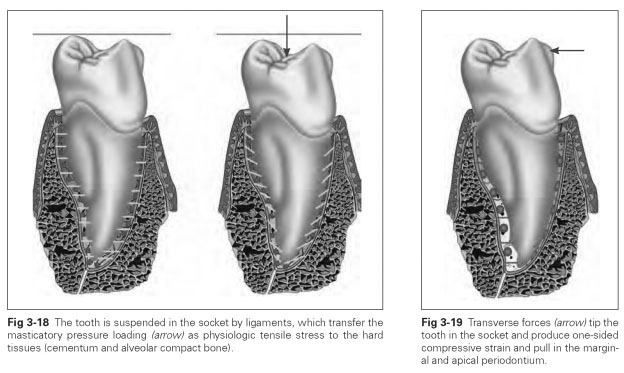
The tooth can also be lifted out of the alveolus to a certain extent; this lifting out is limited by fibers at the apex of the root, which run from the alveolar bone up to the root.The tooth is least secured against tipping movements. A few bundles of fibers do run horizontally and can thereby cushion this movement (Fig 3-19). However, tipping movements can put a strain on the periodontium and damage it because they cause uneven loading. Movements of this kind always occur in connection with masticatory pressure loading where the pivot of the tipping is in the bottom third of the whole tooth.The periodontal ligament is thrust or pulled on one side apically as well as marginally. The physiologic tensile stress has to be cushioned by relatively small areas of the periodontal ligament, which can lead to overloading, while other small surfaces are nonphysiologically compressed. At the same time, a vertical masticatory force has to be absorbed.