Levels of Biologic Intensity
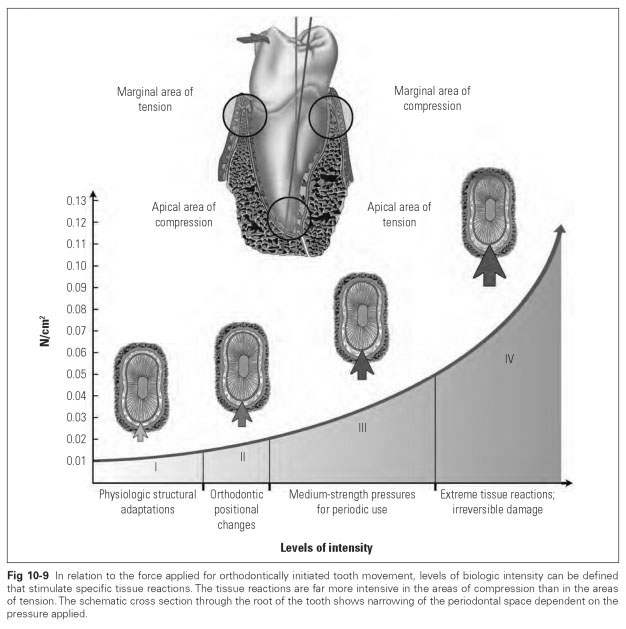
With regard to the amount of force applied to achieve orthodontic tooth movements, four levels of biologic intensity are defined (Fig 10-9).
The first level of biologic intensity has no orthodontic effect. It applies to the operative forces during normal masticatory function and those of the dynamic equilibrium of the tongue, cheeks, and lips, which lead to physiologic structural adaptation.
The second level of biologic intensity arises from weak short-term pressures of 0.015 to 0.020 N/cm2, which are not suitable for fully restricting the 0.1-mm periodontal space or stopping the blood flow. However, these forces can initiate orthodontically effective changes of position.
The third level of biologic intensity is achieved by medium-strength pressures of 0.02 to 0.05 N/ cm2. Capillary blood pressure is surpassed, but the tissue of the periodontal ligament is not fully constricted. These forces are too high for continuous use. Orthodontic appliances exerting this level of force have to be removed for a while after a wearing period of 8 to 12 hours. Otherwise, the fourth level of biologic intensity may ensue.
The fourth level of biologic intensity is achieved by forces that are even higher and are applied continuously. The cells in the areas of compression display irreversible damage after the force is applied for only 2 hours; changes in cellular tissue appear after only half an hour. The blood circulation is stopped, cell membranes rupture, cell nuclei disintegrate, and the cells start to die. After 2 days of continuous application of force, the tissue of the periodontal ligament is dead in the areas of compression. This extreme tissue reaction is seen only rarely in the areas of tension.
In the area of compression, the
alveolar bone cannot be broken down by the dead cells of the periodontal ligament but is resorbed by the deeper-lying cancellous bone cells. Therefore, it takes about 3 weeks for the bone tissue and the dead cells from there to disintegrate. Orthodontic tooth movements are halted for that amount of time. Only afterward is new bone and periodontal ligament tissue formed, and the movement thrust can be reapplied. During such powerfully enforced changes of tooth position, resorptive processes also occur in the cementum of the area of compression, and these processes often spread to the dentin. Initially, only lateral parts of root walls are resorbed, but as the thrust continues, the root apex is resorbed and irreversible shortening of the root by several millimeters occurs. Under normal masticatory pressure, the shortened periodontium is permanently overloaded, the root continues to be resorbed, and the tooth is prematurely lost. Biologically favorable and hence orthodontically effective forces of the second level of biologic intensity promote tissue remodeling that does not leave any irreversible damage.
The first tissue reactions to the application of biologically tolerable force occur in the periodontal ligament as numerous fibroblasts develop. They cause alternating dissolution and formation of new connective tissue fibers. At the same time, bone resorption is stimulated in the areas of compression if the blood circulation is not constricted and cell activity remains intact. The first osteoclasts appear after only 24 hours.
In the area of tension, a layer of osteoblasts starts to form new bone layers after 2 to 4 days. In the process, the stretched straight fibers of the periodontal space are enclosed. Normally the cementum resists bone resorption in the area of compression; it only forms new cementum in the area of tension.
In the case of rotating tooth movements, remodeling processes of much greater magnitude are required in the fibrous system. If a tooth is rotated, the areas of tension are more extensive than the areas of compression. The bundles of fibers must be broken down and new bundles formed, which takes significantly more time than the formation of new alveolar bone. This results in loosening of the tooth, but this is clinically difficult to detect.
Remodeling processes of the marginal fibrous systems need more than a year to reconstruct their functional processes. Sometimes reorientation is not achieved and the straightened tooth reverts to its initial position. When correcting severely rotated teeth, surgical resection of the fibrous systems of the marginal periodontium may become necessary so that the formation of new connective tissue structures is enforced and the tooth is prevented from rotating back again.