Mucosal Covering in the Maxilla
The whole of the palatal area can be occupied by a denture base wherever there is a bony support underneath. In the area of the palatal folds, the palatal mucosa is firm and, without submucosa, is fused to the bone over a wide area; it is permeated by a latticework of collagen fibers and elastic fibers, which gives the palatal mucosa a high degree of strength and deformability.
In the posterior part of the palate, the mucosa is softer and has a submucosa with fatty and glandular tissue in addition to elastic fibers. The palatine glands (glandulae palatinae) guarantee the slidability of the mucosa. With age, these mucosal glands become increasingly replaced by fat.
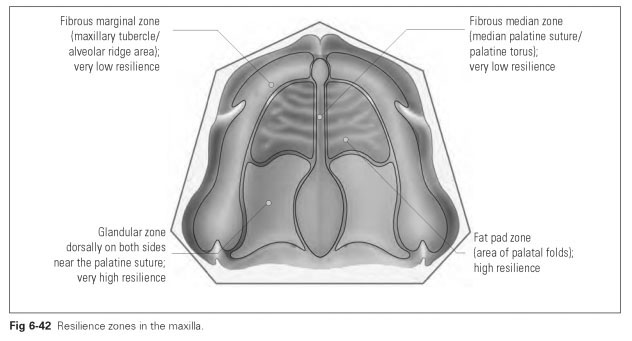
The mucosa can be compressed to varying degrees on its bony base; it is elastic and resistant to stress. It forms pads that are elastic under pressure and act like water cushions. These areas of varying compressibility can be referred to as resilience zones.These variably resilient zones of mucosa (Fig 6-42) include the following:
- The fibrous marginal zone is the area of the alveolar ridge. Here the outer layer of mucosa is firmly fused to the periosteum. The zone is broad at the front, becomes narrower dorsally, and has very low resilience.
- The fibrous median zone is the median palatine suture with the torus from the incisive foramen to the posterior nasal spine. The mucosal layer here is also fused to the periosteum with connective tissue fibers. This zone has very low resilience.
- The glandular zone lies in the dorsal part of the palate near the median palatine suture and has very high resilience.
- The fat pad zone is the pressure and fricative field of the palate, generally the area of palatal folds with relatively high resilience.The fatty tissue is distributed over the whole of the palatine vault, except in the fibrous zones.
- The maxillary tuberosity, as part of the fibrous marginal zone, has very low resilience.
- The incisive papilla is compressible but sensitive.
- The vestibular fornix cannot be described in terms of its resilience because it only has bony support at the infrazygomatic crest.
The very yielding glandular and fat pad zones allow a denture to sink in more markedly when loaded by masticatory pressure. These areas do take on prosthetic significance if so-called etchings are to be made on the denture base.
The transition from hard to soft palate, namely the vibrating line, is particularly important. This borderline is difficult to locate clearly. However, if the soft palate joining the bony palate at this point is made to vibrate by the nose-blowing effect or by pronouncing a vowel during the impression-taking process, the precise course of the border can be traced.
The course of the border runs in an arch from one tuberosity to another. In 90% of cases, this arch is curved dorsally because of the pronounced posterior nasal spine. The vibrating line then runs in a double arch from one tuberosity to another, passing through the two pronounced palatine foveolae (foveola palatina) and enclosing the posterior nasal spine.
The muscle attachments and paths of the cheek and lip muscles also have to be taken into account. Thus, the orbicular muscle of the mouth, the levator and depressor muscles of the angle of the mouth, the greater zygomatic muscle, and the buccinator form a knot of muscles lying in the region of the angle of the mouth. If a canine is incorrectly positioned or the occlusal height is too small, the angle of the mouth will fall inward, which produces a crease in the mouth through which saliva escapes. The corners of the mouth become moist and can become inflamed.
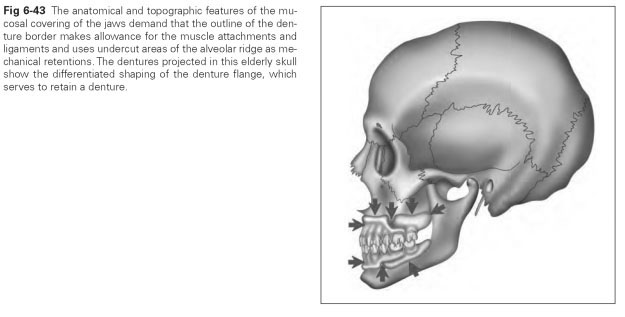
The muscle attachments and course of the muscles in the area of the anterior teeth above the vestibular fornix are strained if the edges of the denture are too overhanging, so that the mucosa in the lip area is pulled inward, the redness of the lips disappears, and a narrow oral fissure results. In addition, a thick denture flange will raise the outer mouth above the upper lip; it looks as if the patient has a roll of cotton wool in the fornix. As well as the feeling of tightness and the altered appearance, pressure points can also develop. To ensure that correct edge shaping is achieved, the impression of the functional edge must allow for the attachment of the buccinator in the tubal/ buccal cavity and in the area of the subjugal crest (Fig 6-43).