Remodeling Processes in Tooth Movement
It is possible to carry out orthodontically induced tooth movements because the dental attachment apparatus with all its tissue structures is capable of constantly renewing itself and adapting to functional changes. These tooth movements require accelerated, very active remodeling rates in the
periodontal ligament and in the hard tissues, especially in the jawbone. In an analysis of remodeling processes, a distinction is made between physiologic
tooth mobility, physiologic tooth migration, and therapeutic changes of tooth position.
Physiologic tooth mobility has the following advantages during normal masticatory function:
- The masticatory forces can be distributed to the rows of teeth.
- The blood supply is guaranteed via shifts in the volume of the network of vessels.
- The rate of renewal of the periodontal tissue is stimulated.
This tooth mobility will not result in any permanent change of tooth position. Physiologic migration of teeth relates to changes in the position of individual teeth in the
alveolar process, and it occurs in two directions:
- Mesially as physiologic mesial migration due to altered approximal contacts
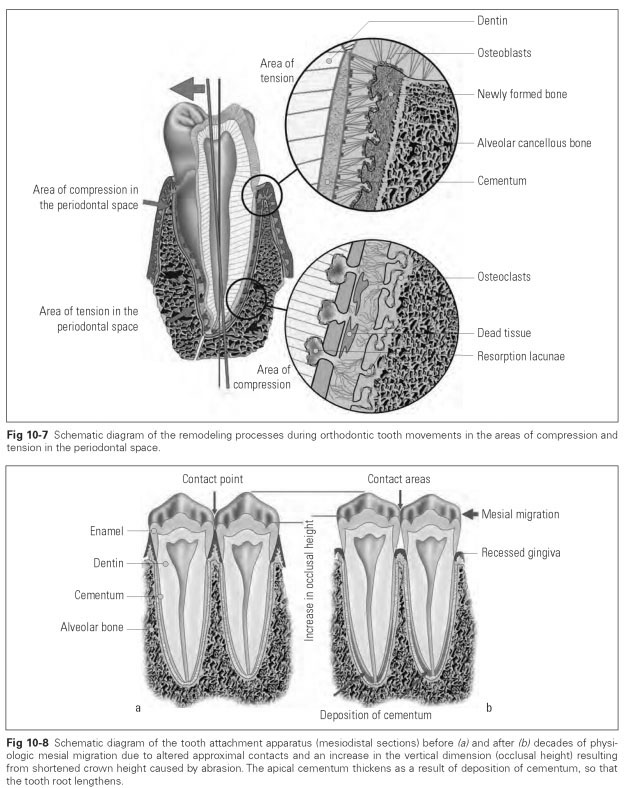
- Occlusally during eruption phases or due to occlusal contacts altered by abrasion (see Fig 10-8)
Artificially produced tooth movements caused by orthodontic appliances are enforced by forces of differing strength. Changes of tooth position in all planes of space are possible. The tissue reactions at the cellular level are the same for both physiologic tooth migration and orthodontic tooth movements.These are complex, biologically controlled adaptive processes of the different cell structures:
- Bone renewal and bone resorption is carried out by osteoblasts, osteocytes, and osteoclasts.
- The periodontal ligament is remodeled by the activity of fibroblasts, as are the connective tissue fibers of the marginal periodontium.
- The cementum is broken down and built up by cementoblasts.
Mesial migration is driven by the permanent tensile forces of the circular ligamentous apparatus. These forces are still effective even if a tooth has been removed from the dentition; the adjacent teeth slowly tip into the gap.
Remodeling processes in mesial migration start with the resorption of all mesially located bone walls in the tooth sockets and with the laying down of bone mass on all distal alveolar walls (Fig 10-7). On the mesial walls, small bulges appear, with many osteoclasts particularly notice-able.Thin layers of bone are deposited on the distal walls. At the same time, remodeling processes take place in the periodontal ligament and the connective tissue of the marginal periodontium. The cementum shows new layers of cement on the distal walls with interposed fibrils for the fiber bundles of the periodontal ligament.
Increases in occlusal height to compensate for abraded chewing surfaces mainly occur due to bone substance being laid down in the depth of the alveolus or due to increases in the apical cementum (Fig 10-8). The driving force for an increase in occlusal height may be a combination of the tension from the fibers of the periodontal ligament and the lifting force of the hydrostatic vascular pressure in the periodontal space, which already raises the tooth out of the socket in normal circumstances.
The force applied must not exceed a biologically tolerable degree if significant damage is to be avoided, such as permanent tooth loosening due to widening of the tooth socket, death of the periodontal ligament tissue, and resorption of tooth roots, which can lead to tooth loss. The biologically most favorable and hence orthodontically optimal force must not exceed the pressure of the capillary blood vessels and lies between 0.02 and 0.03 N/cm2.
Although histologic reactions are essentially the same in response to orthodontically controlled movements, the reactions are stronger depending on the distances of the movements and the degree of force. The following considerations are significant:
- Strength of the force and the lifting movement
- How long the force is applied
- Whether force is applied intermittently or continuously
- Whether tooth displacement, rotation, or tipping is being attempted